Swiss Report of Decline in Youth Gender Dysphoria Does Not Add Up
Bad science got us into trouble with youth gender medicine. Bad science will not get us out.
In recent months, there have been a rush of publications declaring the end of the era of transgender identification among Western youth—and seemingly backing these claims up with data. The most recent claim came from an article by Swiss journalist Birgit Schmid, who examined declining referral numbers to the Zurich gender clinic and concluded that "the gender revolution is over.” The author bolstered her conclusions with references to two recent American analyses, which used survey data and also concluded that trans and nonbinary identification among young people was in "free fall."
Unfortunately, the American analyses fall apart once proper scrutiny is applied to the numbers, as we demonstrated earlier. Our own analysis of a comprehensive data source showed that the number of trans-identified college youths in the U.S. was at an all-time high the last time it was measured in the spring of 2025.
In this Spotlight, we examine the Swiss Zurich gender clinic data and show that claims of an “end of the gender revolution” in Switzerland are likely premature. We also update our prior analysis of transgender identification on U.S. college campuses with data from graduate schools, reinforcing the possibility of reaching a plateau, but finding no evidence yet of a decline.
We conclude with a reflection on the allure of jumping to conclusions when data, at first glance, appear to support a preferred narrative. Confirmation bias, weak data, and overconfident interpretations are at the heart of the medical scandal that has become synonymous with the field of youth gender medicine. We cannot fight bad science with more bad science. We must commit to rigorous, impartial analysis—and follow the evidence wherever it leads. Currently, we find no reliable evidence of a decline in transgender identification or in the demand for pediatric medical transition in the available data.
I. The Swiss Data
The claims of the "end of the gender revolution" among Swiss youth are rooted in the analysis of the number of pediatric referrals for gender dysphoria/gender incongruence to the Zurich gender clinic. These numbers were reported by the Department of Child and Adolescent Psychiatry and Psychotherapy at the University of Zurich (KJPP) as part of an audit performed by the Health Directorate of the Canton of Zurich, and they were made available to the public during a July 2025 press conference.
As Figure 1, presented at the press conference (translated into English below) shows, referrals to the Zurich clinic rose steadily from 2016, then sharply peaked at 134 in 2021, and later fell to 60 consultations in 2024. The author of the article claiming the "end of the gender revolution" interpreted this pattern as a sign of plummeting demand.
However, there are at least three far more plausible explanations that together account for the reported drop—and none support the notion of declining demand.
Figure 1: Registrations for Gender Incongruence Consultations, Zurich University Hospital, Child and Adolescent Psychiatry clinic 2016–2024

Source: https://www.youtube.com/watch?v=QwyScXRWujo&t=802s
- The analysis fails to account for the emergence of several gender clinics that opened after 2020.
Using Zurich referrals as a proxy for trans identification and/or demand for pediatric transition in Switzerland between 2016 and 2024 is misguided, because after 2020 several additional specialized gender clinics were established to meet growing demand. - The analysis does not account for treatments sought from private providers outside hospital-based gender clinics.
The Swiss healthcare system allows patients to seek care from pediatric endocrinologists outside hospital-based gender clinics. Faced with growing waitlists and/or more extensive "gatekeeping," Swiss teens wishing to transition may seek care directly from "affirming" clinicians outside of established gender clinics. - The analysis shows, at best, a return to pre-COVID levels at the Zurich center only.
Even when the Zurich hospital is considered in isolation, and without accounting for the outflow of referrals to newer centers, the data at best indicate a return to pre-COVID 2019 levels—which are already exceptionally high relative to the historical baseline.
We elaborate on each point below.
a. The analysis fails to account for the emergence of several gender clinics that opened after 2020
The conclusion of a sharp fall in referrals for gender-related distress in youth is based on referrals reported by the Zurich clinic. However, Zurich referral numbers are not a reliable proxy for national demand for pediatric transition in Switzerland. While, prior to 2020, the Zurich clinic functioned as the primary gender identity service for youth in the German-speaking cantons of Switzerland, this was no longer the case after 2020. As explicitly acknowledged by the Chair and Medical Director of the Child and Adolescent Psychiatric Service of the Canton of Zurich, Dr. Susanne Walitza, in 2020 and 2021, several additional centers began to offer specialized services to gender-dysphoric youth, and as a result, the demand for consultations at the Zurich clinic decreased:
“In 2020, we began to support other Swiss cantons to develop their own consultation services. From 2020 and 2021, separate consultation services were available in the German-speaking regions of Basel, Bern, Graubünden, Lucerne, Schwyz and Thurgau. And we can see that, from our perspective, this has already led to a decrease in demand for our own consultations.”
While this statement is not entirely precise—for example, Basel and Bern appear to have offered gender services prior to 2020—its conclusion that the services became increasingly dispersed across multiple clinics after 2020 is directionally accurate. A 2023 study from Bern University Hospital, which surveyed Switzerland's nine largest pediatric hospitals' endocrinology departments, found that all nine hospitals "started offering endocrine care and hormonal treatment to children and youths with transsexualism between 2016 and 2022" and that the centers offering these interventions for more than five years “reported increasing numbers of new referrals.”
Thus, since gender services for adolescents were largely consolidated at the Zurich clinic before 2020 but began to spread across several clinics in subsequent years, particularly after 2020, relying on the number of referrals to a single Zurich center between 2016 and 2024 to claim a drop in overall national demand in Switzerland (or even the German-speaking regions of Switzerland) is invalid.
Unfortunately, the presentation of the data at the press conference—particularly the callout on the right side on the graph, which appeared to suggest representativeness across German-speaking regions without clearly indicating the post-2020 addition of new gender centers—inadvertently encouraged this misinterpretation.
b. The analysis does not account for treatments sought from private providers outside established gender clinics
In addition to hospital-based gender services, Swiss adolescents may seek treatment in private, non-hospital-affiliated clinical settings. Switzerland lacks binding national professional guidelines for pediatric medical transition, and there is no requirement that care be initiated within hospital-based services. Several factors could lead youth to seek care in private settings, including the convenience of being treated closer to home; avoidance of treatment delays common in hospital-based clinics due to long waitlists and rising demand; or the desire to bypass cautious or more restrictive protocols that hospital-based multidisciplinary clinics may follow.
c. The analysis shows, at best, a return to pre-COVID levels, which remain exceptionally high
Looking at the Zurich referrals in isolation, the data are consistent with the interpretation that, following a post-COVID spike in referrals for gender-related distress, the numbers have returned to pre-COVID levels.
The peak number of referrals in 2021 (n=134) likely represented a combination of pent-up demand from 2020, when pandemic restrictions limited access to nonessential services and a possible surge in trans identification among youth during COVID-associated lockdowns. In this context, the decline in gender-related consultations in 2024 (n=60) relative to 2021 represents primarily a return to pre-COVID levels observed in 2019 and 2020.
However, it is important to note that the 2019–2020 "baseline" itself represents historically elevated levels. As the graph below from a study by the Bern University Medical Center in Switzerland demonstrates, Switzerland followed the same trends observed elsewhere in the Western world, with rapidly rising numbers of gender-dysphoric adolescents starting in the mid-2010s. As in the rest of the Western world, most of the referrals were for adolescent females with significant comorbid mental health conditions.
Figure 2: Bern University Hospital, Gender Dysphoria Referrals for Children and Adolescents, 2012-2021

Thus, if we accept the hypothesis of a reduction in referrals to pre-COVID levels, this is a return to a "baseline" that is already markedly elevated compared to historical averages.
Concluding thoughts on Swiss trends
Comprehensive national figures for outpatient visits related to diagnoses of gender dysphoria or gender incongruence are not systematically collected in Switzerland. Without such data, it is not possible to draw definitive conclusions about trends in youth demand for gender transition. However, interpreting a single-clinic decline in referrals as evidence of the "end" of the trend is clearly unwarranted.
This point is further underscored by the available national surgical data that show continued increase—rather than decline—in demand for gender-related procedures for youth in Switzerland after 2021. According to inpatient data from the Swiss Federal Statistical Office that collects inpatient data, the number of gender-related surgeries for adolescents increased from 7 in 2018 to 33 in 2023.
Figure 3: Gender Reassignment Surgery for Adolescents in Swiss Hospitals, 2018–2023

Source: https://www.tagesanzeiger.ch/trans-operation-svp-fordert-verbot-in-der-schweiz-786001359271
Although demand for surgery is not a perfect proxy for overall demand for new gender transitions, as surgeries typically trail initial consultations for gender-related distress by several months to years, these numbers do not lend confidence to the narrative of declining demand.
It is worth noting that, starting in 2024, "gender-related" surgeries for adolescents dropped to only five cases, but that drop resulted from increased restrictions allowing surgical "gender-affirming" procedures for youth at the Zurich hospital only in exceptional cases —rather than from reduced demand. This example further underscores the fact that one needs to thoroughly understand both the data and the context before jumping to conclusions.
In summary, the reduction in gender identity-related adolescent referrals to Zurich University Hospital after 2021 cannot be interpreted as evidence of declining gender dysphoria among Swiss youth—or as evidence of reduced demand for pediatric medical transition in Switzerland. In fact, the reported drop in numbers at the Zurich hospital may be a consequence of factors that stem from rising demand: the ongoing expansion of the number of available gender clinics in the German-speaking parts of Switzerland, as well as increased access to private, non-university-based providers who offer gender transition services to adolescents.
II. Expanded analysis of U.S. college campus data
The Swiss publication proclaiming the end of the "gender revolution" appears to have been inspired by American reporting of a purported "plummeting" of transgender and nonbinary identities among American youth. However, the two recent American analyses, which claimed to have found evidence of such a decline, were deeply flawed, as we demonstrated in our earlier Spotlight.
Briefly, the first U.S. analysis (by Kaufmann) found that, when asked about gender, the number of college students selecting the option "other," rather than "male" or "female" dropped. Kaufmann assumed this meant that the number of trans-identified college students had also dropped. However, as we explained in our critique of Kaufmann's analysis, the assumption that trans-identified youth would select “other,” rather than “male” or “female,” is entirely unsupported. In fact, it is much more likely that, given the three choices, transgender-identified males would select "female," while transgender-identified females would select "male." What does seem plausible is that college students who identify as nonbinary would select "other"—and if that is the case, the analysis may indeed have detected a potential decline in nonbinary identities on college campuses.
The second U.S. analysis (by Twenge) examined responses to “Are you transgender?” and “What is your gender?” from the Cooperative Election Study. However, the analysis relied heavily on statistical weights—a method that can distort results when weights designed for the full sample are applied to small subsamples. As we demonstrated in our critique of Twenge's analysis, the sample included extreme weights, with some respondents effectively counting as 0.0001 of a response while others counted as 15. This makes the results fragile and highly model-dependent, as a small number of heavily weighted respondents can meaningfully shift the headline findings. In this case, the weights overwhelmed the underlying trend, even turning increases in transgender identification in the raw data into apparent declines. Such imputed reductions are therefore highly questionable.
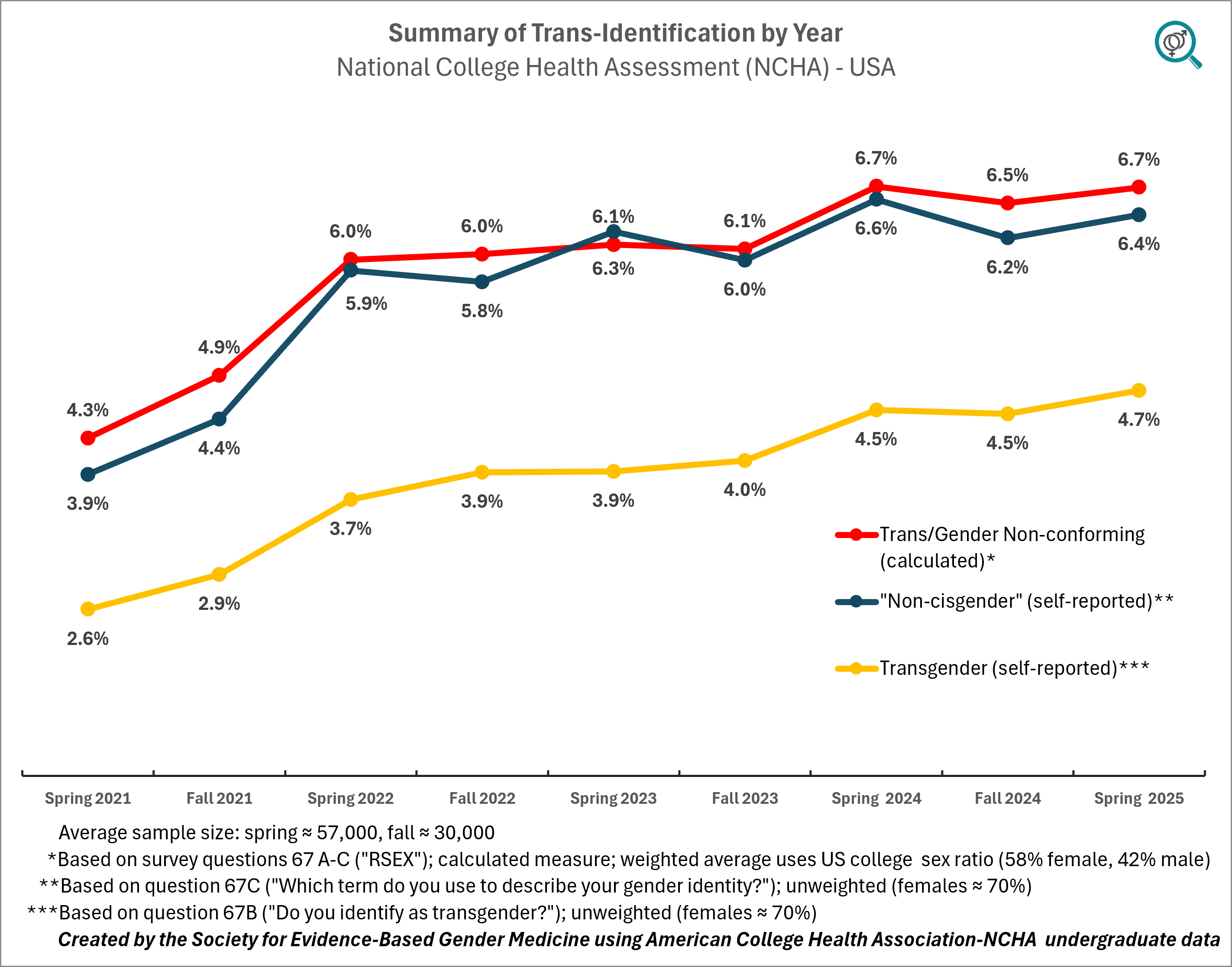
Our critique of Twenge and Kaufmann’s findings was accompanied by our own analysis of transgender identification among youth based on a large probability sample used by the American College Health Association's National College Health Assessment (ACHA-NCHA). ACHA-NCHA has run large surveys every spring and fall since 2000 (about 57,000 respondents in spring and 30,000 in fall, on average). That analysis focused on undergraduate data only.
We found that by spring 2025, transgender identification among college undergraduates reached an all-time high, ranging from 4.7% to 6.7% (margin of error ±0.2%), depending on the method used to estimate trans identification.
Figure 4: Transgender Identification of U.S. College Campuses, 2021–Spring 2025, Undergraduate Report
We have now updated our analysis by adding graduate school data from the same source (NCHA). Like the undergraduate data, the graduate data show that by spring 2025, the percentage of trans-identified graduate students also reached an all-time high, ranging from 2.7% to 4.6% (margin of error ±0.37%), depending on the method used to estimate trans identification.
Figure 5: Transgender Identification on U.S. College Campuses, 2021–Spring 2025, Graduate and Professional Student Report

There is no evidence of a decline in transgender identities in either analysis, although there are early signs of potential stabilization in the undergraduate population. In both graduate and undergraduate populations, the number of trans-identified females continues to significantly outnumber males.
These new results from the graduate and professional student data have been added to the original Spotlight.
SEGM Take-away
The recent claims of the “end” of the era of transgender identification among distressed youth, and of a subsequent decline in demand for youth gender transition, are not substantiated by available data. While we do not doubt anecdotal reports of reduced gender-related distress in youth—and some of us have observed such shifts in our own professional and personal circles—anecdotes do not constitute reliable evidence. Unfortunately, recent analyses put forth to support these claims do not withstand scrutiny.
Just as proponents of pediatric transition too often substituted hope, anecdote, and flawed data for credible analyses that could withstand scrutiny—thereby helping to enable one of the gravest medico-ethical failures of our time—we now see the emergence of similar confirmation bias among some critics of the practice. We are concerned, for example, that viral claims of "plummeting" trans identification among youth in two U.S.-based analyses have been elevated in top-tier popular US publications, while SEGM's robust critiques have been barely acknowledged. As a result, these flawed analyses largely stand uncorrected, and are now unduly influencing similarly-problematic European analyses. This bears a troubling resemblance to the way that "convenient" claims of the benefits of pediatric transitions were rapidly disseminated and influenced policymaking, while devastating critiques of those flawed analyses were known to very few.
We do believe that as patients, parents, the medical community, and society at large become more aware of the serious problems associated with the “gender-affirming” treatment model for youth, overall demand for these services is likely to decline over time. We also expect to see a growing number of analyses suggesting there is evidence for this in the short term. While some reported reductions may reflect a genuine decline in demand—driven by shifting social trends and a growing recognition of the profound problems in youth gender medicine—we should remain vigilant that other reports will simply reflect changes in where and how these interventions are delivered, financed, or in how relevant data are recorded and reported.
We have already demonstrated how survey data can produce unreliable interpretations regarding trends in transgender identification in youth. We now briefly outline how data on medical utilization of gender-related services may also lead to misleading conclusions.
As hospitals reassess their practices and reduce the availability of medical transition interventions, private and less regulated providers may step in to meet demand, producing the appearance of a "reduction" in transitions. Likewise, as some states or countries impose minimum-age requirements or restrict specific interventions—such as the puberty blocker ban in the United Kingdom—affected patients and families may seek care across jurisdictional boundaries, leading to jurisdiction-level reports that overestimate the effect of such policies. Further, high-level data analyses rarely account for workarounds implemented by gender-affirming providers, such as changing billing practices, altering diagnostic coding, or modifying medication regimens to evade restrictions. A portion of both demand and supply may also migrate toward informal or “do-it-yourself” pathways, increasingly facilitated by online communities and direct-to-consumer access to hormones. Finally, because hormones are relatively inexpensive, we expect a shift toward self-financed procedures, which will further undermine insurance-based administrative data analyses.
Finally, it is important to remain alert to one of the most common false signals of “reduced demand” in reports from single hospital-based centers. Following increases in patient demand for youth transitions after 2020 and the development of long waitlists, gender services that were once concentrated in a single prominent clinic began to diffuse across multiple newly opened sites, rendering any one historical center an increasingly unreliable proxy for broader trends. This is what appears to be occurring in Switzerland—and similar dynamics appear to be unfolding in the Netherlands, Australia, and other countries where since 2021–2022 the provision of gender-related services dispersed from a single hospital-based center to multiple providers.
It is incumbent on researchers, clinicians, and other thought leaders to handle emerging data responsibly: to seek to understand the limitations of the data available to them; to maintain a high index of suspicion in the face of “convenient” conclusions; to foreground uncertainty where it exists; and, above all, to resist leaping to conclusions in a rapidly changing landscape.
Our insistence on accurate analysis is not "pedantic." Prematurely declaring the trend over risks lowering scrutiny and redirecting attention just as societies are beginning to grasp the scope of the problem and grapple with ways to mitigate harm in a socially responsible manner. If the ultimate goal is to reduce harm to vulnerable youth, we must hold ourselves to the same evidentiary standards regardless of which conclusions feel most satisfying in the moment.